INTRODUCTION
Elevated intracranial pressure has been associated with increased morbidity and mortality following a head injury1-3). The "staircase" management technique is the normal course of treatment for traumatic brain injury (TBI) patients with raised intracranial pressure; the higher the tier of drugs, the greater the risk of adverse effects and the narrower the benefit-to-risk ratio1,2). Decompressive craniectomy was used to reduce intracranial pressure in some patients with severe traumatic brain injury who were not candidates for conservative treatment4-6). In addition to these commonly used treatments, few studies have looked at the effect of several alternative life-saving therapies with different outcomes7,8). Decompressive laparotomy is one such treatment, and the researchers evaluated its role in improving the outcome of refractory intracranial hypertension in patients with severe TBI9-14). In this study, we conducted a systematic review of the literature and addressed the existing data on the role of decompressive laparotomy in patients with severe traumatic brain injury.
METHOD
The investigation was carried out in compliance with the recommendations of the MOOSE declaration15) for the presentation of systematic reviews of observational studies, meta-analyses, and the Cochrane manual of systematic reviews and meta-analysis16). A search for randomized controlled trial (RCT), not RCT, prospective and retrospective cohort studies will be carried out through PUBMED (until May 2022); SCOPUS (until May 2022); Central Cochrane Registry of Controlled Trials (The Cochrane Library) (until May 2022); MEDLINE (Ovid) until May 2022; EMBASE (Ovid); CINAHL (until May 2022); in addition to the reference list of included studies and other relevant data in addition to potentially eligible studies. The strategy comprised topic headings (MeSH) such as "Decompressive laparotomy," "traumatic brain injury," "Neurocritical care," and "intracranial hypertension," as well as text words associated with Booleans terms. The studies included randomized controlled trials (RCTs), Quasi randomized controlled studies, prospective and retrospective observational studies, series of cases or case reports that employed laparotomy as a therapy for intracranial hypertension. The Newcastle - Ottawa Quality Assessment Scale17) was used to assess the quality of research included; studies with a score of 9 were regarded to have good methodological quality (7 to 9 points). For observational studies, ratings in the range of 6 were considered Moderate Quality, whereas scores of 5 or less were considered Low Quality. The Case quality evaluation throughout CARE check list18) as 13 domains with 30 elements for report. A score of 25 to 30 was classified as High Quality, a score of 18 to 24 as Moderate Quality, a score of 16 to 18 as Low Quality, and a score of 15 or less as Very Low Quality. The following data were retrieved individually and separately: mortality, functional independence (modified Rankin scale 0 to 2, or Glasgow Prognostic Scale with a score of 4 or above), intracranial pressure value before and after Decompressive laparotomy, authors were contacted for missing data. Consultation by consensus helped to clear up any confusion. Statistical analysis was carried out using MEDCAL 19.3 software and the pooled rate of means for grouped data for prognosis evaluation. Because the number of included papers was minimal and this meta-analysis contained case reports, heterogeneity was not addressed.
RESULTS
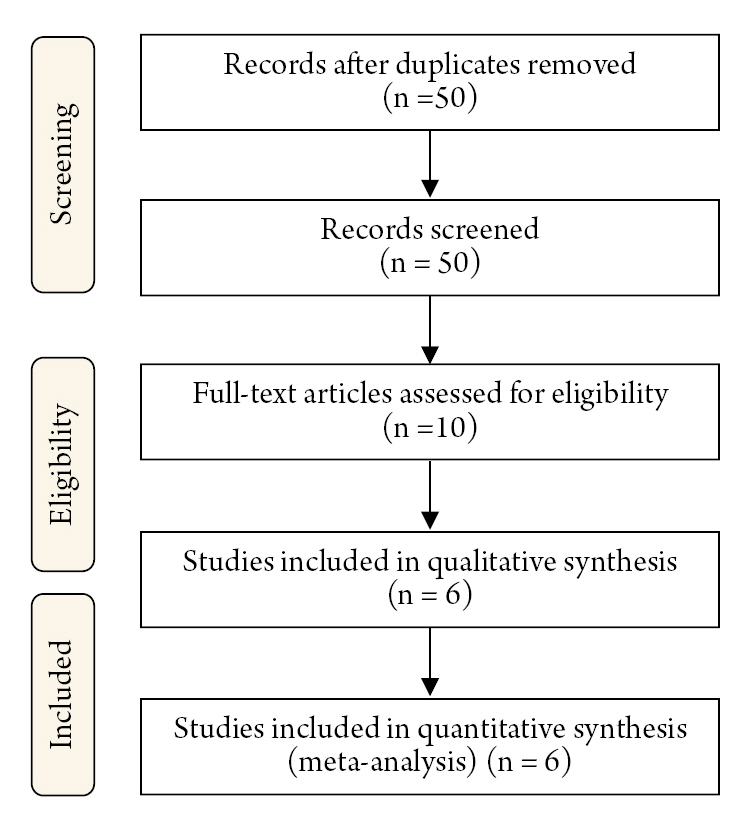
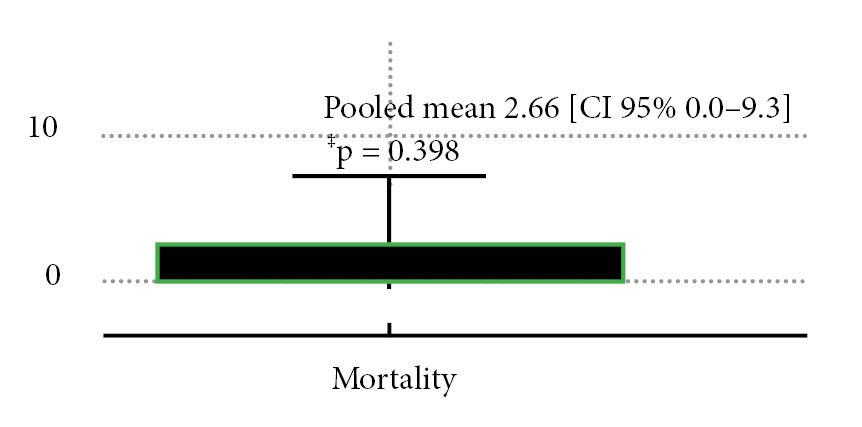
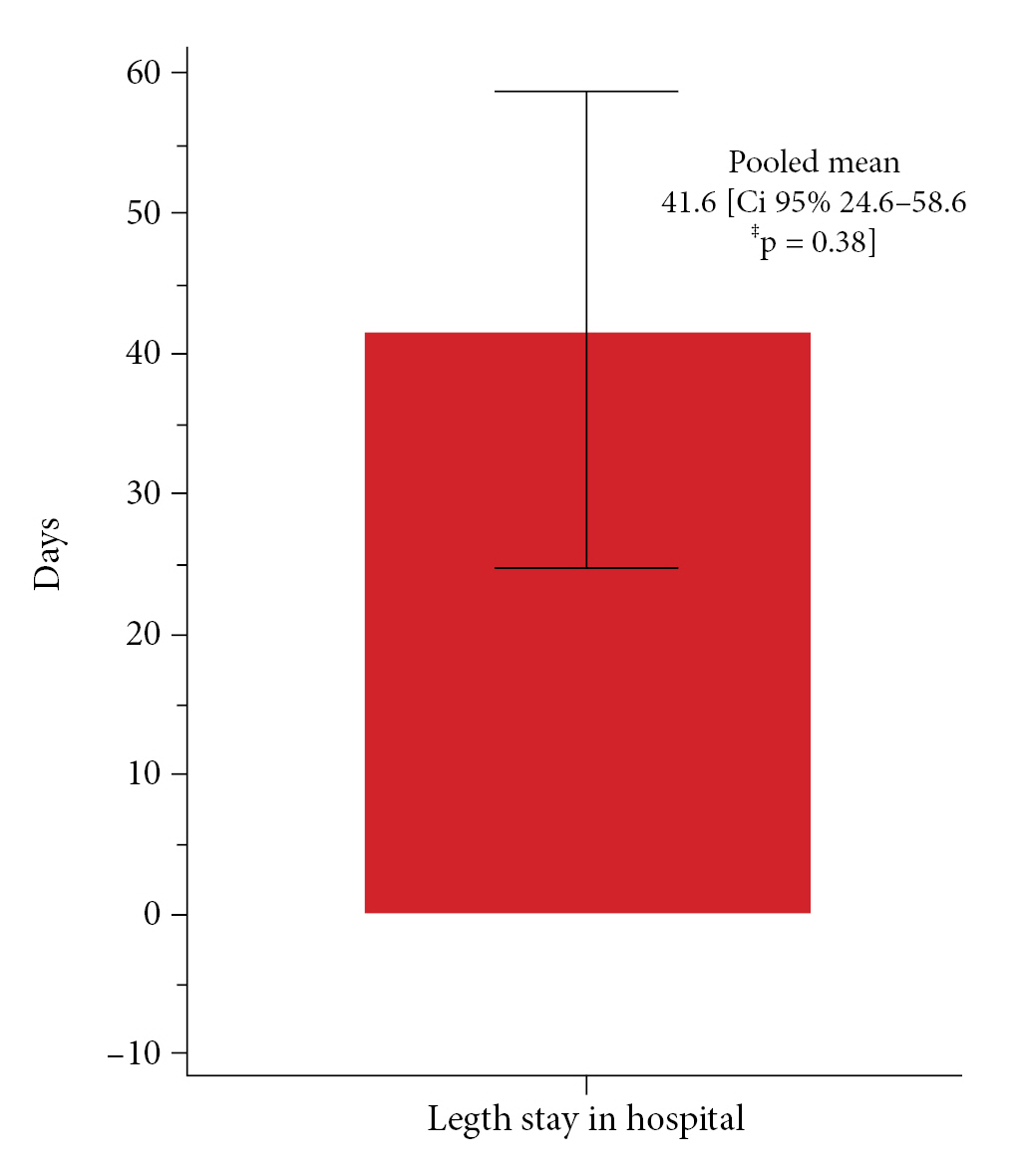
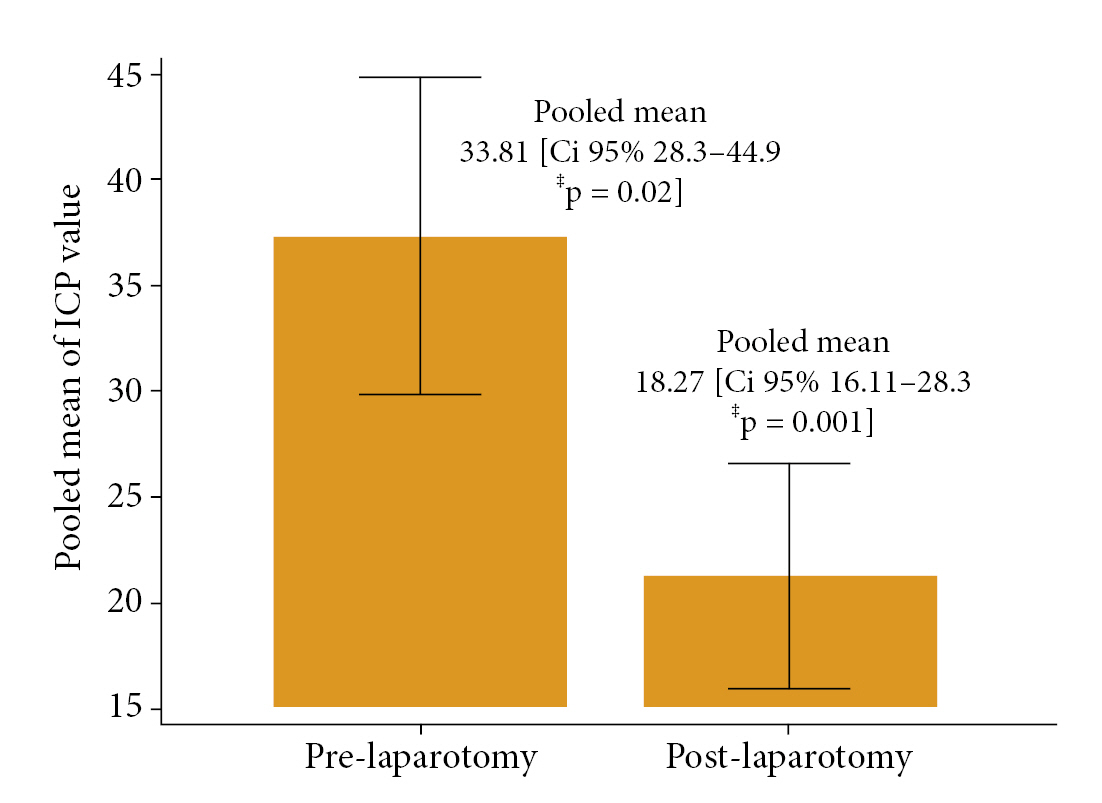
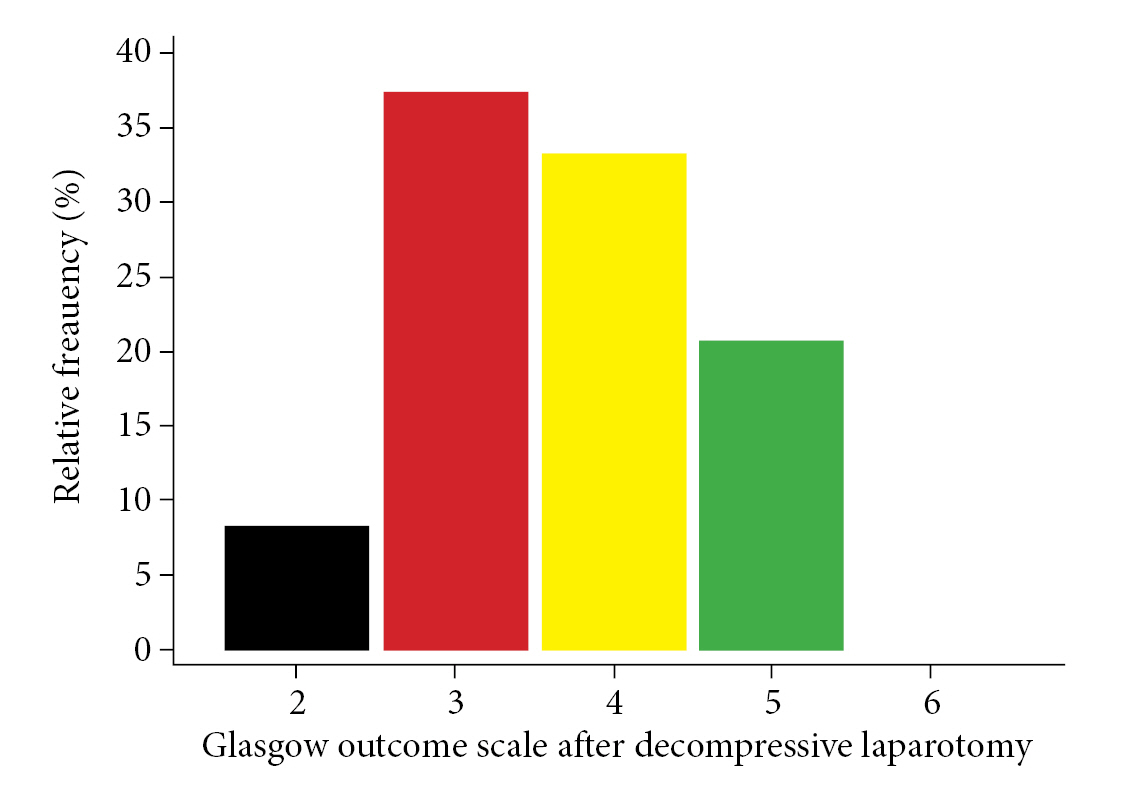
Following our technique of conducting a systematic search for information, 77 bibliographic citations were found. After deleting duplicates, just 50 remained. 50 were identified potentially eligible (based on title or abstract, or both), and complete texts were obtained; 40 were rejected since they were not trauma victims. Following a full text examination, 10 studies were examined for confidentiality: one is a narrative review, two do not contain traumatic brain injury, and one includes thoracic and neck trauma. Six studies were included for qualitative and quantitative analysis. Fig. 1 depicts two observational retrospective cohort studies and four case reports. Tables 1 and 2 illustrate the features of studies included9-14) and eliminated (with reasons)19-22). Among the six trials examined, 46 patients with TBI and intracranial hypertension were assessed and treated with hyperosmolar treatment and/or Decompressive Craniectomy with Decompressive laparotomy. Mortality was defined as death at the end of follow-up; no statistically significant results were identified among patients who underwent decompressive laparotomy, with a pooled mean of 2.66 deaths (Mean 2.66 CI95% 0.0-3.3 p = 0.398) (Fig. 2). The pooled mean of the days in this meta-analysis revealed a long hospital stay of 41.6 days (95% CI 24.6 to 58.6 p = 0.38) with no statistical significance (Fig. 3). After performing a decompressive laparotomy, the mean intracranial pressure drops to normal levels. Pre-laparotomy 33.8 mm Hg measured (95% CI 28.3 to 44.9 p = 0.02) and post-laparotomy 18.24 mm Hg measured (95% CI 16.11 to 28.3 p = 0.0001). All patients’ ICPs were assessed with an external ventricular shunt device (Fig. 4). The Glasgow Outcome Scale was used to assess neurological prognosis and functional competence. According to the findings, 8% of the patients were in a chronic vegetative state, 37.93% had severe disability, 33.45% had moderate disability, and the majorities (64.3%) were able to return to work with limitations, while 20.6% had mild disability or good functional recovery (Fig. 5). Only two observational studies were considered, Joseph et al. 12) and Scalea et al14), which received 5 and 6 points on the Newcastle Ottawa scale, respectively, indicating poor and intermediate quality. The quality of the included case reports was assessed using the CARE Check list. Armanious et al. 10) and Al-jehani et al. 9) are high quality case reports, meeting 28 and 27 quality criteria on the CARE list, respectively. Miglietta et al. 13) 22 met 22 out of 30 criteria, yielding a case report of intermediate quality.
DISCUSSION
Improving outcomes requires prompt care of intracranial after severe TBI1,2). Head elevation, sedation, osmotherapy, decompressive craniectomy, barbiturate coma, and therapeutic hypothermia are all listed as ways to regulate high intracranial pressure, either alone or in various combinations7). The feasibility of decompressive laparotomy has been investigated in selected patients with refractory intracranial hypertension12,13,21,22). The concept of decompressive laparotomy in situations of intractable intracranial hypertension is based on the little evidence that suggests intracranial, intra-thoracic, and intra-abdominal pressures are all connected9-14,19-22). It is postulated that increased intra-abdominal pressure causes cephalad diaphragm displacement, resulting in increased intrathoracic pressure and central venous pressure, which is then conveyed to the cerebral cavity via the venous system14,20,23,24). The authors suggested in a case report that a patient who had numerous traumas (including severe TBI) and underwent large transfusion developed refractory cerebral hypertension that responded to abdominal compartment syndrome laparotomy (ACS) 25-27). Other studies have found that individuals who received high-volume fluid resuscitation were more likely to develop ACS, and that in these cases, refractory intracranial may respond to surgical abdominal decompression25-27). Overall, the decision to pursue aggressive surgical surgery in instances of intractable intracranial hypertension requires careful consideration10,13,14). Decompressive laparotomy had been investigated as an alternative to decompressive hemicraniectomy in patients with bilateral disease necessitating bilateral hemispheric craniectomy or a bifrontal craniectomy, with the expectation that it would be a surgery with less overall morbidity9,14). In cases of recalcitrant cerebral hypertension, decompressive laparotomy must be performed with caution due to the significant morbidity and mortality9,10). To support the basic premise, writers developed methods to evaluate intraabdominal pressure and thereby connect the findings with measurements of intracranial pressure10).