Spinal Cord Reperfusion Injury after Decompression of Severe Cord Compression: Critical Care Management
Article information
Spinal cord injury presentation to intensive care can be due to acute traumatic events, peri-operative injury, controlled surgical trauma to fix the spinal metastatic process, or perfusion limitation with exiting compression. One aspect which is not clear about the presentation is the perfusion of the spinal cord after chronic severe compromise if relieved1,2). Patients have symptoms and signs of spinal cord limitations for a certain period followed by imaging which confirms the compromise. A surgical decision is made upon multiple factors including the severity of symptoms, progression of spinal cord compression, and findings on the imaging. Here we describe a new concept of spinal cord focal reperfusion injury after a chronic severe compromise is partially relieved via endoscopic decompression.
A 44-year-old male with a history of T8-9 disc bulge for 6 months presented to our intensive care unit with new BLE weakness after undergoing a right lateral endoscopically guided T8-9 microdiscectomy at an outpatient surgical center. His symptoms started 6 months ago with numbness of the right leg with no weakness. His symptoms before surgery were urinary retention, perineal numbness, erectile dysfunction, and right flank numbness. An MRI was done before the surgery showing at the T8-T9 level a 13 × 9 × 13 mm extramedullary extradural lesion which was favored to represent a partially calcified disc herniation (Fig. 1A and Fig. 2B). A repeat MRI of the thoracic spine on admission to the intensive care unit showed significant central canal stenosis and evidence of cord compression which is displaced towards the left and posteriorly within the spinal canal. There was evidence of cord signal abnormality suggesting cord edema (Fig. 1B and Fig. 2B). His right leg strength was limited to antigravity, he was not able to bear weight and his sensory deficit was to both superficial and deep touch. The reflexes were markedly reduced. The management for the acute spinal cord injury started with fluids, MAP goal of > 85 mmHg for 72 hours, Dexamethasone and Minocycline. The next day he felt a little better with increased strength in the right leg, not able to weight bear, and getting rehabilitation in the bed. On the third day, the MAP goal was relaxed and fluids were stopped. He was able to bear weight and take a few steps. The steroids were weaned off and Minocycline was restricted to a total of 7 days. He was discharged to the stroke unit followed by acute neurological rehabilitation. A formal and written informed consent was obtained from the patient for the publication of the case information and images.

T2 Axial FLAIR, Sagittal sections. (A) Centered at the T8-T9 level there is a 13 × 9 × 13 mm extramedullary extradural lesion, partially calcified disc herniation. (B) Interval resection of a described via a right transforaminal approach. Fluid and hematocrit layers in the resection cavity, which approximates the size of the resected lesion.
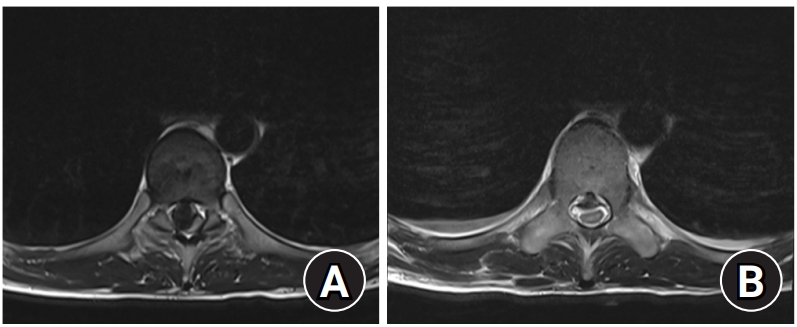
T2 Axial FLAIR, transverse section. (A) Significant central canal stenosis and evidence of cord compression which is displaced towards the left and posteriorly within the spinal canal. (B) Mass effect on the cord remains severe though intramedullary edema at the level of the lesion is more obvious.
Hyperperfusion is a phenomenon that is seen when circulation is provided after perfusion was limited for some time3,4). The best example seen in neurocritical care is the middle cerebral artery hyperperfusion after internal carotid artery stenosis corrective procedure5). Here we notice a reperfusion injury or central spinal cord edema due to relief of severe single-level compression. There is no intraoperative injury noticed and patient improvement was seen within a few days to be able to stand and take a few steps. This process will require further confirmation with an experimental severe subacute focal cord compression. Meanwhile, clinicians should consider this phenomenon in chronic severe focal spinal cord pathologies.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.