Endovascular Treatment Strategies for Vertebral Artery Dissection: A Single-Center Experience and Literature Review
Article information

Abstract
Although some vertebral artery dissection (VADs) cases heal naturally, others progress to stroke, necessitating intervention. Endovascular treatment (EVT) has gained prominence as a viable approach for addressing VADs owing to its perceived low risk of procedure-related complications and high effectiveness. In this review, we share our practical experience of this technique by incorporating the indications and methods for VAD treatment via EVT. Our EVT strategies covered the management of both ruptured and selected cases of unruptured VADs. Unruptured cases that require treatment include those complicated by lesions with recurring or progressive ischemia, large dissecting aneurysms with mass effects, early changes in the VAD structure during follow-up, and involvement of the basilar or bilateral vertebral arteries (VAs). In cases of ruptured VADs, we aimed to occlude the site of rupture through either VA occlusion or stent-assisted coiling. For unruptured VADs, the goal is to restore the original blood flow dynamics using a range of stenting techniques. The choice of EVT technique should be made on a case-by-case basis, considering factors such as the patient's presenting symptoms, hemodynamic status, adequacy of collateral blood supply, and anatomical characteristics of the important arteries and perforators.
INTRODUCTION
Intracranial vertebral artery dissection (VAD) is the most common form of brain arterial dissection. While some types of VAD heal naturally, others progress to stroke and require treatment. Stroke caused by VAD can present as brainstem dysfunction, cerebellar infarction, or subarachnoid hemorrhage (SAH)1). Spontaneous intracranial VAD can be categorized into three primary clinical types: headaches, non-hemorrhagic ischemic symptoms, and SAH2). Arterial dissection begins with sudden disruption of the internal elastic lamina and media, leading to the accumulation of blood within the arterial wall and the formation of an intramural hematoma. In patients with arterial dissection exhibiting a narrowed or blocked arterial pattern, a subintimal hematoma and intimal flap can restrict blood flow3,4).
Endovascular treatment (EVT) has recently gained popularity as a treatment option for VADs because of its low rates of procedure-related complications and high efficacy2,5-7). The choice of treatment for patients with VADs depends on the patency of the contralateral vertebral artery (VA) and the location of the dissection segment in relation to the origin of the posterior inferior cerebellar artery (PICA). Complete occlusion of the dissected segment has been deemed the optimal treatment for VAD5-8). If the dissection is located proximal or distal to the PICA without contralateral VA hypoplasia, the lesion can be treated through complete occlusion of the dissected segment using coils (internal trapping), to allow for PICA filling from the contralateral or ipsilateral VA9). However, when VADs involve the PICA origin, complete isolation of the dissected segment can be achieved through internal coil trapping with PICA revascularization via bypass surgery or PICA stenting. In such cases, EVT techniques such as VA trapping with VA-PICA stenting, multiple stenting, flow-diverting stenting (FDS), and stent-assisted coil embolization (SAC) have shown promising outcomes. In recent years, we have developed and refined strategies for VAD treatment. In this article, we aim to share our experiences with VADs, including their indications and EVT methods.
DIAGNOSIS
Inclusion criteria
(1) A history of acute clinical symptoms and/or signs relevant to intracranial VAD; (2) angiographic evidence of VAD (such as aneurysmal dilatation of the intracranial VA, pearl-and-string signs, or tapered steno-occlusion); and (3) available results from digital subtraction angiography (DSA), magnetic resonance (MR) imaging, and/or computed tomographic (CT) angiography conducted at symptom onset.
Exclusion criteria
(1) Definitive traumatic VAD; (2) iatrogenic VAD; (3) incidental discovery of asymptomatic fusiform dilatations of the VAs; (4) laboratory or angiographic findings suggestive of vasculitis or fibromuscular dysplasia; or (5) lack of documented MR or CT angiography at the initial assessment.
TREATMENT INDICATIONS
We performed EVT for intracranial VADs based on the following indications:
(1) Ruptured VADs with SAH.
(2) Unruptured VADs:
• VAD with recurrent or progressive ischemia
• Dissecting aneurysms > 7 mm, or those causing mass effects
• Early unfavorable changes in VAD morphology during follow-up
• Involvement of the basilar arteries
• Bilateral VADs
Ruptured VADs presenting with SAH
VADs presenting with SAH are considered unstable and carry a high risk of rebleeding, as the hemodynamic stress exerted on the vessel wall can lead to episodes of rebleeding. One study reported a rebleeding rate as high as 71.4% in a group of 42 untreated patients10). In cases of rebleeding, the mortality rate was notably elevated to 46.7%10). EVT can reduce hemodynamic stress and create a favorable environment for healing. The optimal approach for patients with SAH due to VADs involves complete isolation of the dissected segment from the circulation.
Unruptured VADs
Currently, there is no consensus regarding the optimal management strategies for unruptured VADs. Nevertheless, EVT has gained preference as a treatment option for VADs owing to the significant risk of cranial nerve palsy and brainstem injury associated with microsurgery. Intracranial VADs can lead to narrowing and subsequent occlusion of the VA, resulting in thromboembolic ischemia1). Ischemic strokes in the posterior fossa involving the brainstem may lead to elevated mortality rates and substantial morbidity, resulting in a variety of neurological deficits11). Moreover, patients presenting with ischemic symptoms tend to have less favorable outcomes compared to those without such symptoms12). These findings suggest that EVT for VADs during the acute phase should predominantly focus on preventing the progression or recurrence of ischemic stroke (particularly in patients presenting with ischemic symptoms), rather than solely aiming to prevent SAH.
While most unruptured VADs can spontaneously heal, unruptured VADs subsequently leading to SAH have been reported13-15). Large dissecting aneurysms greater than 7 mm or with mass effect and lesions with adverse changes in shape and size during follow-up are associated with an elevated rupture risk. Therefore, EVT is advisable for patients with progressive ischemia or recurrent ischemic symptoms despite medication, as well as for those with an enlarged dissection aneurysm observed on follow-up angiographic imaging16-19).
In the case of unruptured VADs, involvement of the basilar artery appears to hold significant clinical importance in terms of patient outcomes. Previous studies have consistently demonstrated that VADs affecting the basilar artery are independent predictors of unfavorable outcomes12,20-23). Additionally, other factors such as the initial severity of ischemic symptoms (as indicated by a higher baseline National Institutes of Health Stroke Scale [NIHSS] score), dissections involving bilateral VAs, and intracranial VA involvement, have all been suggested as predictors of unfavorable outcomes in cases of unruptured VADs. Consequently, considering EVT for VADs involving the basilar artery, as well as those affecting both VAs seems reasonable12,24,25).
ENDOVASCULAR TREATMENTS
Periprocedural management of antithrombotic therapy
Treatment of ruptured VADs generally involves the administration of loading doses of clopidogrel (300 mg) and aspirin (300 mg), delivered through a nasogastric tube following femoral artery puncture26). Post-procedural surgical management procedures, such as external ventricular drainage and ventriculoperitoneal shunt insertion, can be performed without interruption by antiplatelet agents.
For symptomatic unruptured VADs, patients are administered daily doses of 75 mg clopidogrel and 100 mg aspirin for more than 5 d before undergoing EVT. During the procedure, patients received an intravenous heparin load of 50 IU/kg immediately after guiding catheter placement, and the activated clotting time was maintained at twice the baseline level throughout the endovascular procedure. Heparin administration was discontinued immediately after completion of the procedure. In the event of thromboembolic complications during the procedure, an intra-arterial injection of 0.5–1.0 mg of the glycoprotein IIb/IIIa antagonist tirofiban is administered. After the procedure, patients who have undergone EVT with stents are prescribed daily doses of 75 mg clopidogrel for 3 months, and 100 mg aspirin daily for a minimum of 12 months. Patients previously taking anticoagulants continued to receive the same anticoagulant along with aspirin (100 mg/d). In cases involving FDS, patients were prescribed clopidogrel 75 mg daily for at least 6 months, and aspirin 100 mg daily for at least 24 months. Follow-up angiography is typically scheduled within one month, 3–6 months, and at 12–24 months for unruptured VADs. For symptomatic unruptured VADs, follow-up angiography was conducted at 3–6 months, and then at 12–24 months.
Endovascular techniques
Treatment decisions and endovascular treatment techniques are summarized in Fig. 1.

A flowchart for the treatment decisions and endovascular treatment strategies for vertebral artery dissection. PICA: Posterior inferior cerebellar artery, VAD: Vertebral artery dissection, VA: Vertebral artery.
Deconstructive technique
A deconstructive technique refers to occlusion of the parent artery achieved through methods such as internal coil trapping or proximal coil occlusion. This approach effectively halted blood flow into the dissected segment of the VA. If dissection is not completely excluded from the forward arterial circulation after proximal occlusion, a potential for rebleeding remains. Furthermore, rebleeding can occur if the dissection cavity expands following proximal occlusion. Ideally, the dissected segment should be occluded both proximally and distally to prevent the risk of rebleeding through retrograde filling of the dissecting aneurysm. Deconstructive techniques are preferred and offer advantages for treating ruptured VADs, as they can effectively prevent rebleeding, reduce the likelihood of recurrence, and allow for additional surgical procedures, including external ventricular drainage and decompressive surgery, as no antiplatelet medication is necessary. Deconstructive techniques carry the risk of ischemic stroke in cases where the collateral blood supply is insufficient; therefore, this method is recommended for VADs in nondominant VAs, or VAs with robust collateral circulation.
1)VA trapping (occlusion) by coiling
If dissection occurs either proximal or distal to the PICA, without any significant narrowing (hypoplasia) of the contralateral VA, the lesion can be completely occluded using coils. In this approach, the PICA can subsequently receive blood flow from either the contralateral or ipsilateral VA. Our preferred method was VA trapping by coiling, which involves sacrificing the VA to completely isolate the dissected segment from the circulatory system. Typically, this method is applied to VADs that do not involve the PICA origin in the non-dominant VA using either internal coil trapping or proximal coil occlusion. Proximal occlusion of the VA entails the placement of coils in the segment proximal to the VAD, effectively blocking blood flow into the affected region. Conversely, internal coil trapping involves the embolization of the VA within the dissected segment itself. In cases where a deconstructive method was considered for dominant VAs, we performed balloon test occlusion at the ipsilateral VA, proximal to the affected segment, to assess the feasibility and safety of the procedure.
2) VA trapping (occlusion) with PICA stenting
When VAD involves the origin of the PICA in the nondominant VA, a substantial risk of PICA infarction is incurred if internal coil trapping is performed6,27). In the context of EVT, the preferred approach in such a case is reconstructive therapy. In our practice, occlusion of the dissected segment by coil embolization, while preserving the PICA through PICA stenting, was considered. We have previously reported a case in which we treated a patient with a self-expanding closed-cell Enterprise stent (Codman Neurovascular, FL, USA) deployed from the proximal VA to the PICA. We thereby achieved complete occlusion of the dissected segment through coiling (Fig. 2)6). When the origin of the PICA involves the distal segment of the VAD, we may perform internal coil trapping of the VAD and PICA stenting by deploying an Enterprise stent from the distal VA to the PICA, by approaching from the contralateral VA7).
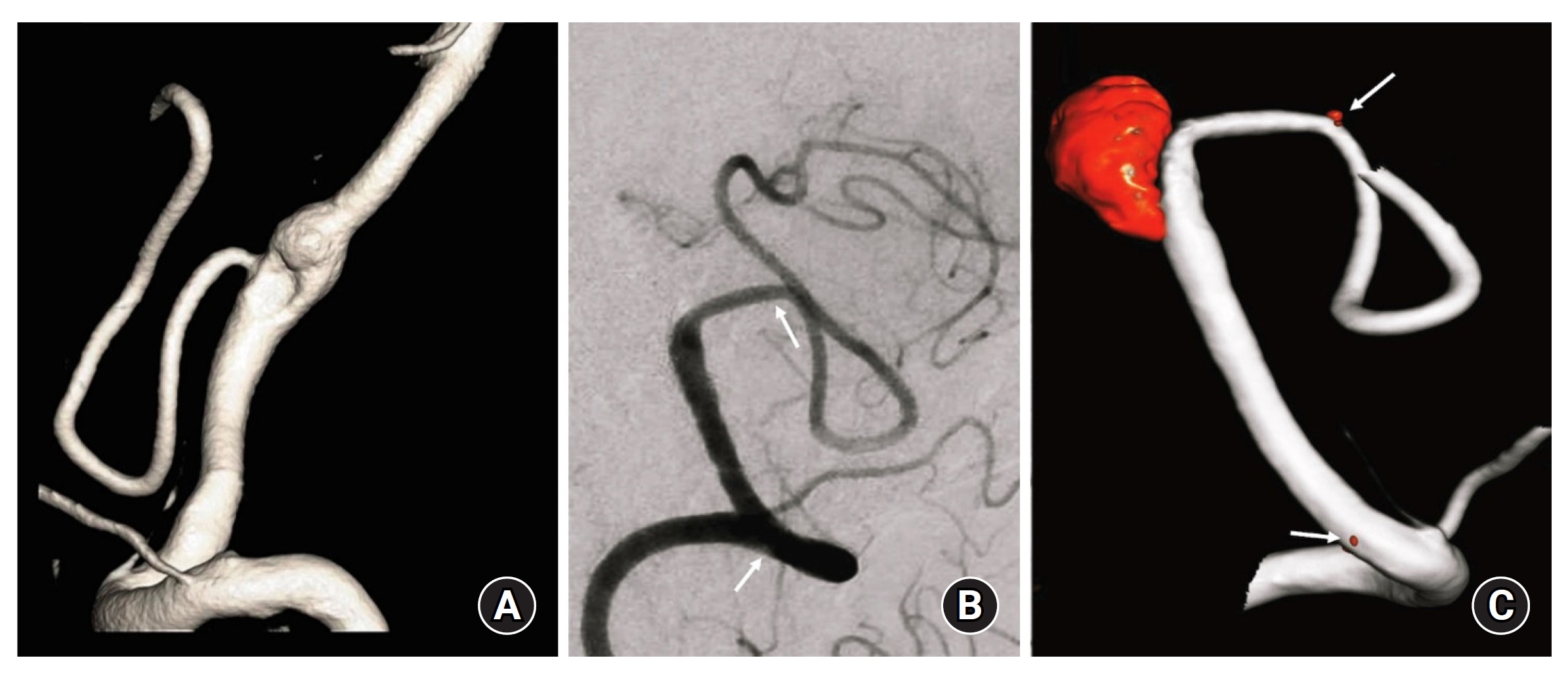
(A) Three-dimensional reconstruction image showing a ruptured vertebral artery dissection with involvement of the origin of the posterior inferior cerebellar artery (PICA) in a non-dominant vertebral artery (VA). (B) One-year follow-up angiography. (C) Three-dimensional reconstruction image showing PICA patency. Arrows indicate proximal and distal stent markers in the VA and the PICA.
When we assessed the clinical and radiological outcomes of VADs involving the PICA origin using different EVT approaches (VA trapping with VA-PICA stenting, multiple stenting, SAC, and FDS), we found that VA trapping with VA-PICA stenting resulted in the lowest recurrence rate and favorable neurological outcomes. In contrast, SAC displayed higher recurrence rates and a high potential for severe, disabling infarctions5).
Regarding PICA patency following VA-PICA stenting, we have previously shared our experience using Enterprise stents in small arteries (less than 2 mm in diameter)28). Among the 31 enrolled patients, three (9.7%) experienced procedure-related complications, all of which were asymptomatic. Follow-up angiography was performed in 27 patients (87.1 %) at an average of 15.5 months post-EVT. In cases where the parent arteries had two acute angles (four cases), 75.0% were occluded on follow-up angiography. Conversely, parent arteries with either no acute angles (13 cases) or one acute angle (six cases) showed 100% patency on follow-up angiography. Further, a significant difference was found between the sizes of the parent arteries at follow-up and before EVT (p=0.037). On multivariate logistic regression analysis, the tortuosity (number of acute angles) of the parent arteries was identified as the sole predisposing factor for size increments of the parent arteries on follow-up angiography. Successful stent navigation and deployment were achieved in all patients (100%) without symptomatic procedure-related complications. These results suggest that the angiographic configuration and course of the parent arteries are crucial factors in maintaining the patency of parent arteries with a diameter of less than 2 mm. Thus, stent deployment in small parent arteries is technically safe. Based on our findings, we believe that PICA patency can be ensured following VA-PICA stenting.
Reconstructive technique
Deconstructive techniques may not always be feasible, especially in cases of VADs involving the dominant or solitary VA with limited collateral blood flow, or in instances of bilateral VADs. In such scenarios, reconstructive techniques that aim to preserve the parent artery by using stents alone or in combination with coiling have gained prominence as viable alternatives for vessel deconstruction. Reconstructive techniques offer potential benefits, particularly in cases in which complete angiographic occlusion is not the primary goal. Endovascular reconstruction of VADs employing methods such as multiple stenting (the stent-in-stent technique), SAC, and FDS have also become more common. The objective of these techniques is to prevent ischemic complications, while restoring the original hemodynamics of the affected artery. Notably, all reconstructive techniques require an extended period of dual antiplatelet therapy, particularly in the context of SAH, which may pose challenges for subsequent neurosurgical interventions, such as external ventricular drainage and craniectomy. However, reconstructive techniques offer the advantage of maintaining physiological blood flow in the ipsilateral VA, which may reduce the risk of periprocedural morbidity. Understanding the relationship between the dissected segment of the VA and critical structures such as the anterior spinal artery, PICA, and medullary perforators is of utmost importance to ensure a safe and enduring cure following EVT.
1) Multiple stenting
In cases of symptomatic unruptured VADs or lesions with steno-occlusive angiographic features such as the pearl-and-string sign, multiple stenting is often considered. When a self-expanding closed-cell stent is deployed to cover the dissected segment, it facilitates the reconstitution of the vessel lumen. This, in turn, aids in the stabilization of the intimal flaps, and promotes vessel wall repair by encouraging neointima formation. In instances where the VAD extends over a very long segment and reaches the basilar artery without the presence of a large dissecting aneurysm, employing multiple stents with a telescoping technique can prove to be an effective treatment method. We prefer using a laser-cut closed-cell Enterprise stent for multiple stents. This technique was found to be easy to deploy and exhibited a commendable chronic outward force, indicating its ability to maintain its diameter against external forces. Moreover, when using a closed-cell-design stent and opting for oversizing, the stent tends to possess a higher chronic outward force29).
One approach we employed for multiple stenting without coiling, particularly when VAD occurred in the dominant or solitary VA, was the double-stenting technique. This method involves deploying a Low-profile Visualized Intraluminal Support (LVIS) Blue stent (Microvention, Tustin, CA, USA) within an Enterprise stent29). LVIS Blue stent is a braided stent known for providing a high degree of metal coverage, typically ranging from 22–28%. This characteristic makes the LVIS Blue stent beneficial for achieving complete obliteration of a dissecting aneurysm, as it enhances the occlusion rate by exerting a flow diversion effect. Moreover, the overlapping LVIS Blue stents can potentially act as flow diverter devices because of their substantial metal coverage surface area. However, deploying an LVIS Blue stent in a VAD may result in a reduced metal coverage surface area, as the device often experiences a transition from a constrained to an unconstrained diameter30-32). To overcome this limitation and capitalize on the flow diversion effect of the LVIS Blue stent, we utilized the structural properties of a laser-cut closed-cell Enterprise stent using a technique known as the LVIS Blue stent-within-an-Enterprise stent. The Enterprise stent exhibited minimal outward expansion at the unconstrained segment, and served as a scaffold to reduce the size of the unconstrained segment across the fusiform dissecting aneurysm neck. This ensured an even distribution of high metal coverage surface area and porosity without the presence of a transition zone at either end of the aneurysm neck. Consequently, the flow-diverting effect of the LVIS Blue stent remained intact. An Enterprise stent typically provides a metal coverage surface area ranging from 8 to 11%. After overlapping with the LVIS Blue stent, the metal coverage surface area increased to approximately 33% of the straight vessel. Using this technique, we were able to facilitate the complete obliteration of VA dissecting aneurysms, while promoting endothelial healing of the VA (Fig. 3)33). This technique offers a cost-effective alternative to deploying dedicated flow diverters. In addition, the delivery and deployment processes are relatively simple and straightforward. However, this technique requires an adequate time for complete healing of the dissected segment. Therefore, it may not be suitable for ruptured VADs, given the challenge of achieving immediate obliteration of the rupture point and the associated risk of hemorrhagic complications due to the use of dual antiplatelet agents during the acute phase.

(A) Right vertebral artery (VA) angiography showing the dissecting aneurysm involving 360 degree of the dominant VA. (B) Flow stagnation inside the aneurysm immediately after performing a LVIS blue stent-within-an-Enterprise stent technique. (C) Right VA angiography at 6-month follow-up revealing complete obliteration of the aneurysm and remodeling of the VA. The VA shows good patency without in-stent stenosis. White arrowheads and black arrowheads indicate proximal and distal ends of the LVIS Blue and Enterprise, respectively.
2) Stent-assisted coiling
In cases involving ruptured VADs associated with dissecting aneurysms within the dominant or single VA with limited collateral flow, multiple stenting or FDS may present a risk of rebleeding during the latent period when the dissecting flap stabilizes and thrombosis forms within the dissecting aneurysm. Owing to the non-saccular shape of the dissecting aneurysms, reconstructive techniques without coils are often challenging for ruptured VADs. As a result, our preferred approach for patients with ruptured VADs and aneurysmal dilatation in the dominant or single VA was the SAC (Fig. 4).

(A) Ruptured bilateral vertebral artery dissections with dominant vertebral artery (VA) on the right. (B) Right dominant VA had fusiform aneurysmal dilatation with the rupture point on the inferior part. (C) Left non-dominant VA was occluded by internal coil trapping and stent-assisted coiling with triple stenting was performed for the right dominant VA. (D) Follow-up angiography at 12-month showing complete obliteration of the dissecting aneurysm and well-reconstruction of right dominant VA. A white arrow indicates the anterior spinal artery is originated just distal to the issecting aneurysm.
However, when performing SAC for VADs, considering the involvement of critical branches such as the anterior spinal artery, PICA, or medullary perforators is crucial. Preserving these branches is paramount for safe reconstruction of the VA. In some cases, achieving complete SAC may be challenging, as dissecting aneurysms frequently exhibit fusiform rather than saccular dilatation. In such instances, if the rupture point of a dissecting aneurysm is identified, the coils can be packed densely into that specific area. SAC of VADs involving the PICA tends to experience a higher recurrence rate than other treatment options. One study conducted by Cho et al. assessed the clinical and radiologic outcomes of VADs involving the PICA based on different types of EVT5). They observed that both the multiple stenting and VA-PICA stenting groups had the highest rate of postoperative infarction, followed by the SAC group. However, no infarction occurred in the FDS group during the follow-up period. Furthermore, dissecting aneurysm recurrence was noted in 25% of patients treated with SAC, probably because a strategic decision was made to leave a small portion of the dissecting aneurysm to ensure patency of the PICA.
To spare these critical branches originating from the VA, two LVIS Blue stents partially overlapping in the dissecting segment can be deployed, ensuring that the proximal and distal segments of the VA are covered by a single stent. This approach helps reduce the risk of perforator infarction from the normal VA segment, and enhances the flow-diverting effect to increase the chances of complete healing of the dissecting segment.
3) Flow diverting stenting
Reconstructive procedures involving FDS have become the preferred choice worldwide and are gradually replacing multiple stenting procedures (Fig. 5). One notable advantage of FDS is its potential to preserve the patency of branching vessels and perforators originating from the parent artery34-38). The presence of gaps between the stent strands facilitates blood flow into these branching vessels, while simultaneously disrupting flow into the dissecting aneurysm and promoting intrasaccular thrombosis. Recent meta-analyses have reported a perforator infarction rate of approximately 3%, with a slightly higher rate observed in patients with posterior circulation aneurysms compared to those with anterior circulation aneurysms39). The concept of wall reconstruction appears logical when considering a ruptured VAD as a diffuse defect of the vessel wall. However, comprehensive multicenter studies of the outcomes of these reconstructive techniques are limited. Most outcome data are derived from published case series38,40-43). As the use of FDS for VADs continues to grow, larger studies are warranted to determine long-term outcomes, including aneurysm occlusion rates, thromboembolic complications resulting from device insertion, and consequences of covered branch vessels and perforators.
(A) Digital subtraction angiography of the left vertebral artery showing vertebral artery dissection (VAD) with a dissecting aneurysm. (B) A 6-month follow-up angiography showing complete healing of the VAD after treatment with a flow diverting stent, Pipeline Flex with Shield technology. Although the flow diverting stent covered the origin of the posterior inferior cerebellar artery (PICA), the flow of the PICA was patent.
DISCUSSION
EVT has emerged as the preferred treatment for intracranial VADs. However, a consistent and universally accepted strategy for determining when to reconstruct or occlude an affected VA segment has yet to be established. In this article, we share our real-world practices and experiences accumulated over the past decade in the treatment of VADs using EVT. Our approach was based on the specific clinical situation and anatomical characteristics of each patient. In cases of ruptured VADs, we generally occluded the rupture point by performing VA occlusion in the non-dominant VA or SAC occlusion in the dominant VA. For unruptured VADs, VA reconstruction using various stents is considered to maintain the original hemodynamics.
Notably, the current trend in treating VADs leans towards reconstructive techniques using FDS. However, it is essential to recognize that reconstructive techniques involving stents, particularly for ruptured VADs, pose the risks of procedure-related complications and recurrence. In a previous study, we reported our experience with SAC for ruptured wide-necked aneurysms in the acute period, and assessed the incidence and risk factors of procedure-related complications26). Among 72 patients treated with SAC, we found a periprocedural complication rate of 19.4%. The overall procedure-related thromboembolic complication rate regardless of symptoms was 12.5%, which exceeded the risk of hemorrhagic complications. Based on these findings, we concluded that microsurgical clipping or alternative endovascular techniques, such as the multiple-microcatheter or balloon-assisted technique, may be more appropriate first-line treatment options than SAC, particularly for patients with poor clinical grades or acute hydrocephalus. Furthermore, we evaluated the postoperative stroke risk and recurrence rate of both ruptured and unruptured VADs involving the PICA following different EVT modalities6). Our findings indicated that VA trapping with VA-PICA stenting showed the lowest rate of aneurysm recurrence, but was associated with a higher rate of minor infarction and favorable neurologic outcomes. In contrast, SAC is associated with high recurrence rates and a risk of fatal disabling infarction. Importantly, the rate of post-treatment recurrence did not significantly differ between the reconstructive and deconstructive techniques. The involvement of the PICA origin by VADs was identified as the only independent risk factor for recurrence after EVT8). These findings underscore the importance of carefully considering the choice of treatment modality for VADs, the patient's clinical status, anatomical factors, and the potential risks and benefits associated with each technique.
In a prior meta-analysis examining patients with vertebrobasilar dissecting aneurysms treated using either reconstructive or deconstructive techniques, the immediate occlusion rate was found to be 75.0% (95% CI, 55.0–88.0%), while the long-term occlusion rate was 87.0% (95% CI, 74.0–94.0%)44). Additionally, the angiographic recurrence rate was estimated to be 7.0% (95% CI, 5.0–10.0%), with a retreatment rate of 3.0% (95% CI, 2.0–6.0%). The perioperative morbidity rate was 12.0% (95% CI, 9.0–16.0%), and the all-cause perioperative mortality rate was 8.0% (95% CI, 6.0–11.0%). The overall rebleeding rate in patients with ruptured dissecting aneurysms was 9.0% (95% CI, 6.0–13.0%). When comparing deconstructive and reconstructive techniques, we observed that patients treated with deconstructive methods had higher rates of complete occlusion not only immediately after the procedure (88.0% vs. 53.0%, p<0.0001), but also on long-term follow-up angiography (88.0% vs. 81.0%, p< 0.0001). In contrast, perioperative morbidity was lower in the reconstructive group than in the deconstructive group (4.0% vs. 12.0%, p=0.04). Although we observed a trend towards a lower perioperative mortality rate (4.0% vs. 10.0%, p=0.11) and a higher rate of good long-term clinical outcomes (92.0% vs. 86.0%, p=0.10) in the reconstruction group, these differences were not statistically significant. In summary, this meta-analysis suggests that EVT of vertebrobasilar dissecting aneurysms can achieve a high rate of complete occlusion and yield favorable long-term neurological outcomes. Deconstructive techniques may result in a higher rate of complete angiographic occlusion, whereas reconstructive techniques may be associated with lower perioperative morbidity. However, long-term neurological outcomes and retreatment rates were statistically similar between the two treatment modalities.
Radiologically, VADs can be categorized into three groups: dilatation without stenosis, pearl-and-string appearance, and stenosis without dilatation45). In the angiographic evaluation of symptomatic unruptured VADs, aneurysmal dilatation is more common than the steno-occlusive type. This distinction differs from that of extracranial vertebral artery dissection, in which the steno-occlusive type predominates. One possible explanation for this difference in lesion type is the absence of an external elastic lamina and a decreased amount of medial elastic tissue in the intradural artery. Subintimal dissections tend to result in luminal stenosis or occlusion, while subadventitial dissections often result in dilatation. The primary lesion morphology in symptomatic intracranial VADs may differ between unruptured and ruptured cases. Further, the morphology of symptomatic intracranial VADs may change during follow-up imaging. Ahn et al argued that ruptured VADs are more likely to present with dilatation without stenosis or a pearl-and-string appearance than with a stenosis without dilatation apperance45). In their study, intramural hematoma occurred in 33.9% (78 out of 230) of cases, developing most frequently in lesions featuring stenosis without dilatation (42 out of 60 [70%]), followed by lesions with a pearl-and-string appearance (27 out of 90 [30%]), and dilatation without stenosis appearance (9 out of 80 [11%]) (p< 0.05)45). The dilatation-without-stenosis group remained stable in 74% (25 out of 34) of cases, while the stenosis-without-dilatation group showed improvement in 91% (39 out of 43) of cases. Intracranial VADs with intramural hematoma exhibited progression at a four-fold higher rate than VADs without intramural hematoma (20% vs. 5%, p=0.003)45).
CONCLUSION
Determining the optimal course of action for VAD treatment is a complex decision-making process. Nevertheless, EVT is currently the primary approach for managing VADs. The EVT technique should be selected on a case-by-case basis, considering clinical symptoms, hemodynamic conditions (including collateral blood supply adequacy), and anatomical characteristics of the neighboring major arteries and perforators. The decision-making process should be guided by both endovascular neurosurgeons and interventional neuroradiologists.
Notes
Ethics statement
This study was a literature review of previously published studies and was therefore exempt from institutional review board approval.
Author contributions
Conceptualization: SKP, JC. Writing- original draft:JC. Writing, review & editing: JK, SKP.
Conflict of interest
There is no conflict of interest to disclose.
Funding
None.
Data availability
None.
Acknowledgements
None.